About Me
|
About Me
|
Home | About Me | Favorite Links | Contact Me |
 |
Introducing Tristan David Horacek |
|
|
Tricuspid Artresia What is it? In this condition, there’s no tricuspid valve so blood can’t
flow from the right atrium to the right ventricle. As a result, the right ventricle is small and not fully developed. The
child’s survival depends on there being an opening in the wall between the atria (atrial septal defect) and usually
an opening in the wall between the two ventricles (ventricular septal defect). As a result, the low-oxygen (bluish) blood
that returns from the body veins to the right atrium flows through the atrial septal defect and into the left atrium. There
it mixes with oxygen-rich (red) blood from the lungs. Most of this partially oxygenated blood goes from the left ventricle
into the aorta and on to the body. A smaller-than-normal amount flows through the ventricular septal defect into the small
right ventricle, through the pulmonary artery, and back to the lungs. Because of this abnormal circulation, the child looks
blue (cyanotic).
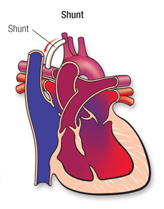
What can be done to treat it? Often
it’s necessary to do a surgical procedure, called a shunt, to increase blood flow to the lungs. This improves the cyanosis.
Some children with tricuspid atresia have too much blood flowing to the lungs. They may need a different type of surgery,
called pulmonary artery banding, to decrease blood flow to the lungs. This is important to protect the lung blood vessels.
This
procedure is done for single ventricle defects that can result in a narrowing of the aorta. The surgery involves attaching
the aorta and pulmonary artery to each other. This ensures that the flood can flow out of the aorta properly so that enough
blood gets to the lungs. Sometimes the aorta is also enlarged during this surgery if it is too small or stenotic, with the Norwood procedure. This is known as aortic reconstruction. The DKS procedure is an open heart procedure. Without
treatment, the majority of children with single ventricle heart disease would die very early in life. Surgical repair is available
and the ultimate goal is survival and improvement of the child's quality and length of life. Unfortunately,
at present, it is not yet possible to recreate the anatomy and function of a normal heart with these particular conditions.
Instead, the goal is to separate the blue and pink circulations of the blood to improve the amount of oxygen in the body and
to decrease the amount of extra work on the one chambered heart. A
hole in the wall between the two upper chambers (ASD) or between the two ventricles (VSD) can cause problems. The severity
of the symptoms depends on the size and the location of the defect and can go from no symptoms at all to severe heart failure.
Heart failure in the infant results in poor feedings (feeding is the most exercise an infant does) and poor weight gain. In the older child, heart failure
may cause decreased exercise tolerance and shortness of breath. Depending
on their size and location, septal defects may close spontaneously. The cardiologist will likely wait a while before recommending
surgical treatment to see if that happens naturally. In cases involving larger holes and severe symptoms, however, treatment
with surgery or catheter closure with a device will be needed, again depending on size and location. The
surgical treatment for ASDs and VSDs is open heart surgery. The heart is stopped and opened, and the hole is sutured with a patch made of a synthetic material like Dacron or a patch of pericardium (the thick sac that surrounds the heart). Complications are minimal and length of stay in the hospital is about three days.
Complications are the ones associated with any open heart surgery plus the possibility of heart block by damage to the heart's conduction system near the hole (1% risk). Another
newer, and not yet widely used approach, involves inserting a closure device (you may see it referred to as a septal occluder)
into the hole through a cardiac catheterization procedure. This stops the blood flow through the septum. A
very new approach to ASD correction is being tested in the U.S. The Columbia Presbyterian Robotic Cardiac Surgery team in
2001 was the first to successfully repair this defect with the help of a robot. The completely closed heart procedure was
done without a chest incision. This approach is currently being tested on other patients as part of a clinical trial approved by the U.S. Food and Drug Administration.
Below are future Surgeries I will need to correct the blood flow from
my heart to my body and lungs. Can it be repaired? Most children with tricuspid atresia can have surgery to allow their hearts to work more like normal. Connections are created
between the body veins and the lung (pulmonary) arteries. This is usually done in two stages. First, the large vein from the
upper half of the body (the superior vena cava) is connected to the lung arteries in a procedure called a Bidirectional Glenn
Operation. Later, the large vein from the lower half of the body (the inferior vena cava,) as well as the veins from the liver, are
connected to the lung arteries in a surgery called a Fontan Operation. Sometimes, at the time of the Fontan surgery,
an opening is purposely left between the bluish (low-oxygen) and red (high-oxygen) sides of the blood flows. The Fontan operation
may eliminate or greatly improve the cyanosis but, without a right ventricle that works normally, the heart doesn’t
work like a normal heart, which has two pumps. The Fontan procedure can be performed using a tube that goes around the
heart as shown in the picture or with a path (baffle) that goes inside the heart. Both types of Fontan operations route the
blue blood from the lower half of the body and liver to the lungs. What will my child need in the future? Children with tricuspid atresia require lifelong follow-up by a cardiologist for repeated checks of how their heart is
working.
Cardiac catheterization (KATH-e-ter-i-ZA-shun) is a medical procedure used to diagnose and treat certain heart conditions.
A long, thin, flexible tube called a catheter is put into a blood vessel in your arm, groin (upper thigh), or neck and
threaded to your heart. Through the catheter, doctors can do diagnostic tests and treatments on your heart. For example, your doctor may put a special dye in the catheter. This dye will flow through your bloodstream to your heart.
Once the dye reaches your heart, it will make the inside of your coronary (heart) arteries show up on an x ray. This test
is called coronary angiography (an-jee-OG-ra-fee). The dye can show whether a substance called plaque (plak) has narrowed or blocked any of your coronary arteries. Plaque
is made up of fat, cholesterol, calcium, and other substances found in your blood. Plaque narrows the inside of the arteries and, in time, may restrict blood flow to your heart. When plaque builds up in
the coronary arteries, the condition is called coronary heart disease (CHD) or coronary artery disease. Blockages in the coronary arteries also can be seen using ultrasound during cardiac catheterization. Ultrasound uses sound
waves to create detailed pictures of the heart's blood vessels. Doctors may take samples of blood and heart muscle during cardiac catheterization and do minor heart surgery. Cardiologists (heart specialists) usually do cardiac catheterization in a hospital. You're awake during the procedure,
and it causes little to no pain. However, you may feel some soreness in the blood vessel where the catheter was inserted.
Cardiac catheterization rarely causes serious complications. Revised May 2009
|
|
|